More misandry from the Guardian
That zombie click-bait rag, the Guardian, has been excelling itself with the misandrist dross it publishes. The article below, written by Alexandra Topping, appeared in the Guardian on December 23rd. Alexandra is yet another Oxbridge English Literature graduate writing for that ‘newspaper.’ A degree in English Literature, particularly from ‘Oxbridge’ apparently makes you an expert on every topic, including health matters – or so Alexandra Topping appears to believe. If you want to read the article, click the image or click here.

Paragraph2 reads – In many countries men face greater health risks, but not in the UK. A study from Manual, a wellbeing platform for men, has found the UK has the largest female health gap among G20 countries and the 12th largest globally.
‘Manual’ is not so much a wellbeing platform aimed at men as an advertising platform promoting supposedly health-giving products such as hair-loss spray and ‘testosterone support’ – not exactly a scholarly or impartial information source. The health gap that is referred to is not the relative health between men and women but the relative international ranking for women’s health and men’s health. The UK does badly for both, but ranks slightly lower for women. It doesn’t mean that women in the UK are faring worse than men. Alexandra knows this of course- it is just typical disingenuous writing from the Guardian. I am not even sure about the reliability of the rankings. The tables are based on a methodology that is opaque.
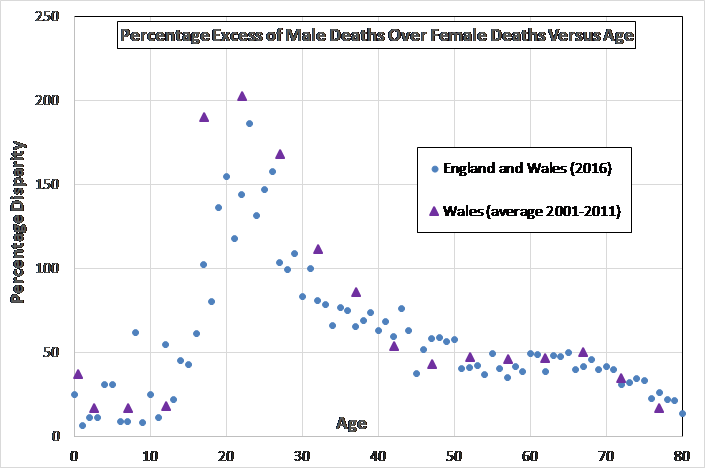
The fact is that men face significantly greater health risks and have a 43% greater chance of dying before 75 compared to women – that is a real gender health gap.
Paragraph 2 – Women, in particular young women, are also more likely to experience common mental health conditions than men, despite the fact that men account for about three-quarters of deaths registered as suicide.
That men are three times more likely to commit suicide is a pretty striking health gap, one that is attributed to toxic masculinity. Meanwhile, I don’t hear anyone attributing higher rates of anxiety and depression among women to toxic femininity (neither should they).
Paragraph 3. The inequalities start well before women make it to their doctor’s surgery. Women are routinely underrepresented in clinical trials, and medical research proposed by women, for women, is not allotted the same funding as medical research proposed by men, for, you guessed it, men.
No data is provided by Alexandra Topping to support this claim. A study published in the British Journal of Pharmacology (here) showed no evidence of the underrepresentation of women in clinical trials. Female participation in phase II and III trials runs at 48%, which is hardly a major difference. Female participation is lower in the more risky phase I trials but no drug gets to market without going through all phases.
Sexism is still rampant in healthcare, not least among staff. Despite the fact the NHS workforce is dominated by women, men working in NHS trusts are still paid more than their female peers.
No evidence is provided to justify the claim that sexism is rampant. Men in NHS trusts, on average, work longer hours and more women choose to work part time. That is what accounts for the earnings gap. It is illegal and has been for over 50 years to pay men or women less for the same job.
Tireless work by the campaigner and writer Caroline Criado Perez demonstrates that, as she states in her book Invisible Women: Exposing Data Bias in a World Designed for Men, healthcare is “systematically discriminating against women, leaving them chronically misunderstood, mistreated and misdiagnosed”.
Caroline Criado Perez is an activist author of a polemical book and not an expert on health matters. Women have not been considered less important in health care. Compare, for example, the spending on women only diseases with that on men only diseases. Breast cancer and prostate cancer is good place to start.
But gender inequality in healthcare runs deep. Recognising, as the government has today, that system-wide changes are needed to tackle “decades of gender health inequality” is a vital first step yet, as Criado-Perez has said, women have been considered less important in healthcare as far back as Ancient Greece.
This is just invective. Gender health inequality primarily affects men. At birth, there are roughly equal numbers of males and females yet the population as a whole comprises 51% when and 49% women. That grim statistic tells you what you need to know, More men die early to result in that discrepancy (see graph below). That is a real gender health gap.
Men’s access to health care is also limited compared to women’s. Although men are blamed for their problems by not visiting the doctor soon enough, the best available data paints a different picture.
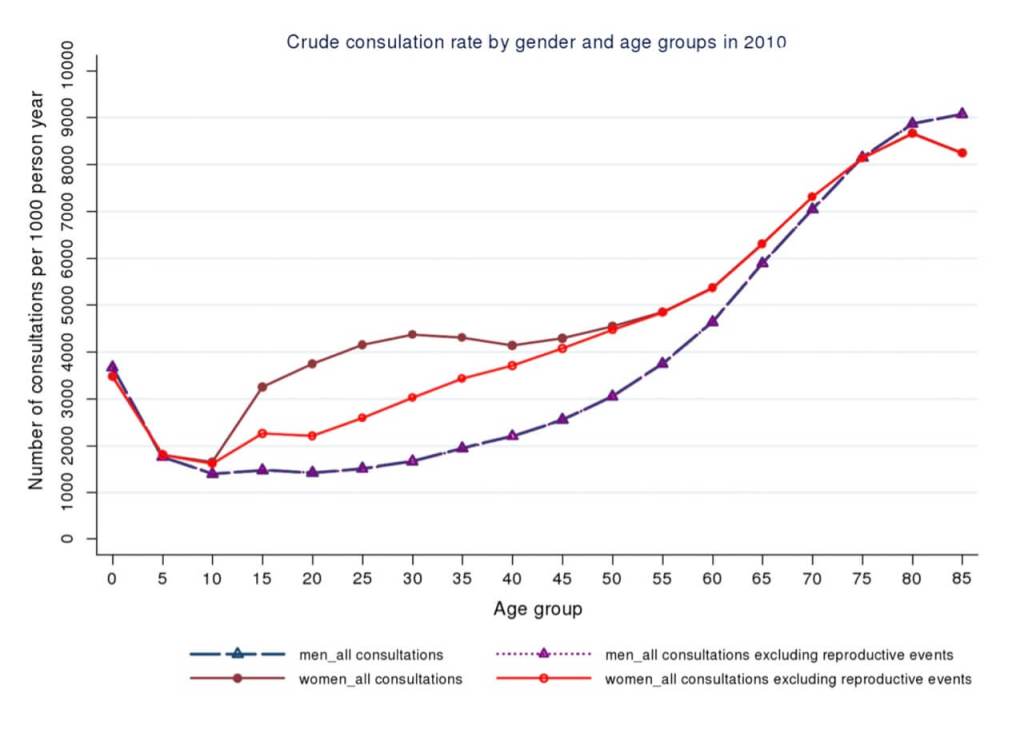
Looking at the graph above you can see that men do indeed make fewer consultations with general practitioners (dashed purple line). This difference gets less once you adjust for consultations around ‘female reproductive events’ (pregnancy?). The striking thing, however, is that this difference only applies to men of working age. Among older and younger men the consultation rate is about the same. What this suggests is that it is men’s working lives that make health care less accessible to them.
A study by Alan White and Karl Whitty (here) looking at men’s underuse of health services found that 80% more men than women work full time in the UK, 50% more women who work full time have flexible working arrangements and three times as many men work more than 45 hours a week. Attending for health checks is more problematic for men than women.
If you look for areas of health provision that disadvantage women you will find them. If you look for areas of health provision that disadvantage men, you will find them. That is only an exercise in confirmation bias. Whether the UK health service is tilted in favour of males or females is a different and much harder question to answer. A toxic zero-sum game where the landscape has to be tilted against men to benefit women benefits nobody.
We should be working hand-in-hand to improve the health service for everybody.

3 comments